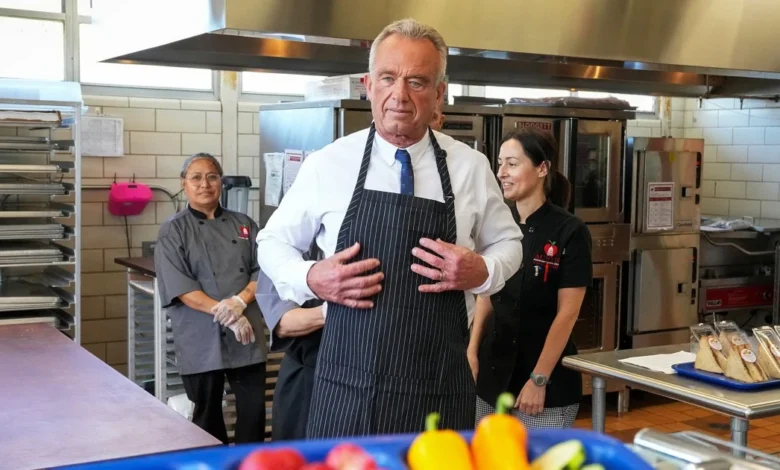
Health Secretary Robert F. Kennedy Jr. has launched a bold initiative aimed at increasing nutrition education in medical schools. His announcement comes after months of persistent pressure on educational institutions to expand their curricula. Kennedy threatens funding cuts for schools that refuse to comply while offering public recognition for those that embrace the initiative. This plan stems from a long-held belief that inadequate training in nutrition leads physicians to prioritize medication over dietary interventions in managing chronic diseases. The announcement coincides with a growing concern among various stakeholders about the adequacy of nutrition training, a conversation that spans decades.
The Coordination of Interests and Strategic Goals
The initiative is designed to probe deeper than simply enhancing educational content; it serves as a tactical hedge against a broader criticism of medical training. Kennedy’s approach indicates an urgent responsiveness to the ongoing dialogue surrounding healthcare effectiveness in the U.S., where doctors often grapple with the implications of nutrition in their practices.
According to senior Department of Health and Human Services officials, 52 medical schools have voluntarily signed on to the initiative, which mandates three key actions: auditing existing nutrition training, appointing a faculty member for oversight, and establishing a public page detailing how they will achieve a minimum of 40 hours of nutrition education for students. This creates a framework without enforcing a rigid curriculum, thus allowing schools to adapt the guidance to their specific needs.
Educational Reforms and Historical Context
A pivotal study published in the Journal of Biomedical Education in 2015 revealed that medical students receive, on average, only 19 hours of nutrition training over four years. This alarming statistic positions Kennedy’s push within a historical backdrop where nutrition has been sidelined in medical education for decades. The American Medical Association has echoed these concerns since the 1960s, indicating that the prevailing model for training physicians often neglects the significance of diet in health management.
Critique arises, however, around the oversimplified notion that expanding nutrition education alone will substantially shift medical practice. Experts like Dr. Adam Gaffney argue that addressing nutritional issues requires understanding financial and social barriers faced by patients rather than merely increasing education hours. This insight reveals a tension between Kennedy’s objectives and the practical realities of healthcare delivery.
| Stakeholder | Before Initiative | After Initiative |
|---|---|---|
| Medical Schools | Limited nutrition curriculum (average of 19 hours) | Potentially enhanced curriculum with focus on nutrition (goal of 40 hours) |
| Students | Lack of nutrition education in training | Increased knowledge and awareness of nutrition’s role in health |
| Patients | Limited nutritional guidance from doctors | Better-informed physicians leading to improved dietary advice |
| Health Policy Advocates | Calls for comprehensive nutritional education largely ignored | Increased attention to policy changes regarding nutrition in medical training |
The Ripple Effect Across Global Markets
This push by Kennedy resonates well beyond U.S. borders. In the UK, Canada, and Australia, similar conversations surrounding medical education and the necessity of nutrition training are gaining traction. As governments and education bodies grapple with healthcare costs and public health outcomes, the integration of nutrition into medical curricula could become a pivotal factor influencing healthcare delivery worldwide. For example, recent debates in the UK regarding health inequalities underline the significant role that diet plays in patient outcomes.
Projected Outcomes: What to Watch For
As this initiative unfolds, several developments warrant attention:
- Increased Participation: An uptick in the number of medical schools adopting the recommendations could reshape future curricula.
- Public Recognition: The promise of recognition for compliant schools may trigger competitive dynamics among medical institutions.
- Shifts in Patient Care Models: A focus on nutritional education may catalyze more holistic approaches to patient care in the coming years.
In conclusion, while Kennedy’s initiative is a vital step toward enhancing nutrition education in medical schools, it raises broader questions about the adequacy of a purely educational response to systemic healthcare challenges. Stakeholders from varied backgrounds will need to engage in meaningful discourse to ensure that this push translates into real-world patient outcomes.